25 year old male with diabetes with generalised weakness of both upper and lower limb
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan
A 25 year old male car driver by occupation and resident of narketpally came to opd with
Chief complaints :
-generalised weakness of both upper limbs and lower limbs since 2-3 months
History of presenting illness :
Patient was apparently asymptomatic 3 months back , then he developed generalised weakness and increase urine output 2 months back
Nocturia since more than 2 months
Then he visited local hospital and after all investigations done he got diagnosed with type 2 diabetes. He was prescribed for regular medication [ metformin ]
After using medication for 10 days , his weakness got subsided
He had 3 episodes of headache in the last 3 months which is diffuse , non radiating , on and off , throbbing type , no aggravating factors , but temporarily relieved on medication
No h/o blurring of vision , Diplopia , photophobia
H/o polydipsia
He has tingling sensation but no numbness in both upper limbs and lower limbs
H/o sob on lying down after meal and relieved on sitting position since 3 months
H/o weight loss of 4 kgs in the last 3 months
No h/o vomitings , loose stools , abdominal distension , constipation
No h/o cough , cold , fever
No h/o Orthopnea , pnd , chest pain
No h/o palpitations , sleep disturbances
No h/o hematuria
Past history :
No similar complaints in past
Not a known case of Hypertension , epilepsy , tuberculosis , asthma , tuberculosis , thyroid abnormalities
No past surgeries
Personal history :
Diet - mixed
Appetite - normal
Bowel and bladder movements - regular
Sleep - adequate
No addictions
No known allergies
Daily routine :

Diet:
Morning | 2 millet roti , bowl of curry | 450 calories |
Afternoon | 2 millet roti with dal or curry | 500 calories |
Night | 2 millet roti with curry | 450 calories |
Total | 1400 calories |
Required calories according to his age - 2400 calories
Calories deficit - 1000 calories
Family history :
His father is a known case of diabetes since 5 years
General examination :
Patient is conscious , coherent , cooperative
Well oriented to place , time , person
Moderately built and moderately nourished
Bilateral mid arm circumference - 12 cm
Abdominal circumference - 35 cm
Vitals -
Bp - 120 / 80 mmhg
Hr - 84 bpm
Rr - 17 cpm
Signs
Pallor - absent
Icterus - absent
Cyanosis - absent
Clubbing - absent
Generalised lymphadenopathy - absent
Bilateral pedal edema - absent





Systemic examination
Per abdomen
Inspection -
Shape of abdomen : scaphoid
Umbilicus : inverted , central
All quadrants of abdomen are moving equally with respiration
No dilated veins , scars , engorged veins , sinuses
No visible pulsations
Palpation -
All inspectors findings are confirmed
No local rise in temperature
Abdomen is soft
No tenderness
No guarding , no rigidity
Deep Palpation- no organomegaly
Percussion -
No shifting dullness
No fluid thrill
Auscultation -
Regular bowel sounds are heard
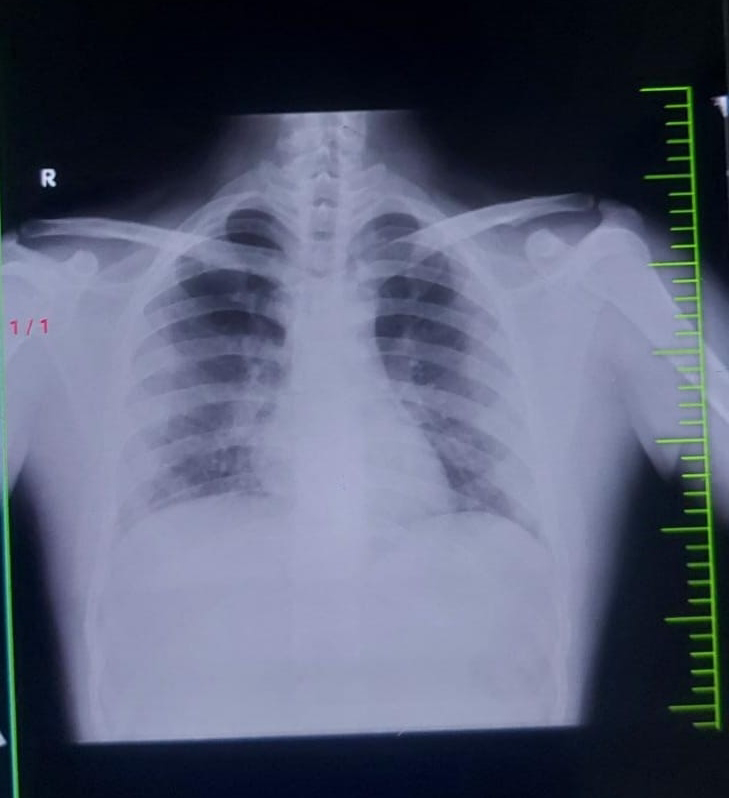
Respiratory system examination :
Inspection -
Chest appears to be bilaterally symmetrical , elliptical in shape
Trachea appears to be central [ midline ] in position
Chest in moving equal and normal with respiration
No sinus , no scars , no dilated veins , no swellings , no drooping of shoulder , no hallowing
Palpation -
All inspectory findings are confirmed
No local rise of temperature , no tenderness
Trachea -midline
Apical impulse is felt
Tactile focal fermitus - appreciated
No palpable swellings , no crowding of ribs
Percussion -
The following areas are percussed
|
Area |
Right |
Left |
|
Supraclavicular |
Resonant |
Resonant |
|
Infraclavicular |
Resonant |
Resonant |
|
Mammary |
Resonant |
Resonant |
|
Axillary |
Resonant |
Resonant |
|
Infraaxillary |
Resonant |
Resonant |
|
Suprascapular |
Resonant |
Resonant |
|
Infrascapular |
Resonant |
Resonant |
Auscultation - bilateral normal vesicular breath sounds are heard
Cardiovascular system :
Inspection -
Chest wall : no abnormalities
No visible pulsations , sinuses , scars , engorged veins
Palpation -
All inspectory findings are confirmed
Position of trachea is central
Apical impulse is felt
No parasternal heave , no tenderness , no rise in temperature
Auscultation -
S1 , s2 hears
No murmurs
No added thrills
Central nervous system examination -
Right | Lower limb | Normal |
Upper limb | Normal | |
Left | Lower limb | Normal |
Upper limb | Normal |
Biceps | ++ |
Triceps | ++ |
Supinator | ++ |
Knee | ++ |
Ankle | ++ |















Comments
Post a Comment