This E blog also reflects my patient cantered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
case presentation -
A 32 year old male patient came to OPD with chief complaints of
-Fever since 7 days
-Stomach pain since 7 days
History of presenting illness -
Patient was apparently assymptomatic 7 days back then he developed fever which is insidious in onset , gradually progressive , high grade fever , increased during night , associated with chills and rigors , no aggravating factors , relieved temporarily on medication
History of night sweats
Then he developed pain abdomen since 1 week which was insidious in onset , gradually progressive , pain in right hypochondrium , right lumbar , umbilical region which was pricking type , non radiating , aggrevated on inspiration , non relieving factor
H/o cough since 3 days insidious on onset , non productive
No h/o post nasal drip , sore throat , running nose , nasal congestion , headache
No h/o constipation , nausea , vomiting , loose stools , abdominal distension
No h/o dypsnea , wheezing
No h/o chest pain , palpitations , pnd,orthopnea , platypnea
No h/o hemoptysis , hoarseness of voice , burning micturition
Past h/o:
H/o of hospital admission in hospital 9 days back , where he was non relieved and came to our hospital
Not a k/c/o hypertension , diabetes , asthma , epilepsy , tuberculosis
Personal h/o :
Diet - mixed
Sleep - disturbed
Appetite - normal
Bowel and bladder movements - regular
Addictions - ocassionally drinks alcohol
No smoking habits
No allergies
Family h/o :
No significant family history
Treatment h/o :
Pleural tap done on 14.04.23 ( 20 ml ) and on 15.04.23 (30 ml )
General examination -
Patient was conscious , coherent , cooperative
Moderately built , moderately nourished
No signs of pallor
Icterus - absent
Cyanosis - absent
Clubbing - absent
Kolionychia - absent
Lymphadenopathy - absent
Edema - absent
Vitals :
Pulse - 86
Bp - 120/ 80 mmhg
Temp - afebrile
Rr - 16 cpm
Systemic examination -
Respiratory :
Inspection -
Trachea appears to Be midline
Chest movements appears to Be equal
Shape of chest appears to Be elliptical
No scars , no sinuses , engorged veins
No hallowing , no crowding of ribs , drooping of shoulder
Palpation -
All inspectory findings are confirmed
No Local rise of temperature
No tenderness
Trachea - central
Bilateral chest movements are equal
No palpable swelling , masses
Vocal fermitus - Rt. Lt
Supraclavicular : N N
Infraclavicular : N. N
Mammary : Decreased N
Inframammary : decreased. N
Axillary : Decreased. N
Infraaxillary : decreased. N
Suprascapular : N. N
Infrascapular : N. N
Interscapular : N. N
Percussion -
Inspection -
Shape of abdomen - appears to Be scaphoid
Umbilicus - appears to Be inverted
No scars , no swellings , engorged veins
No visible pulsations , no peristalsis
Palpation -
Local rise of temperature is seen
Tenderness in right hypochondrium , right lumbar , umbilical region
No mass felt
Percussion -
No h/o fluid thrill , liver span , shifting dullness
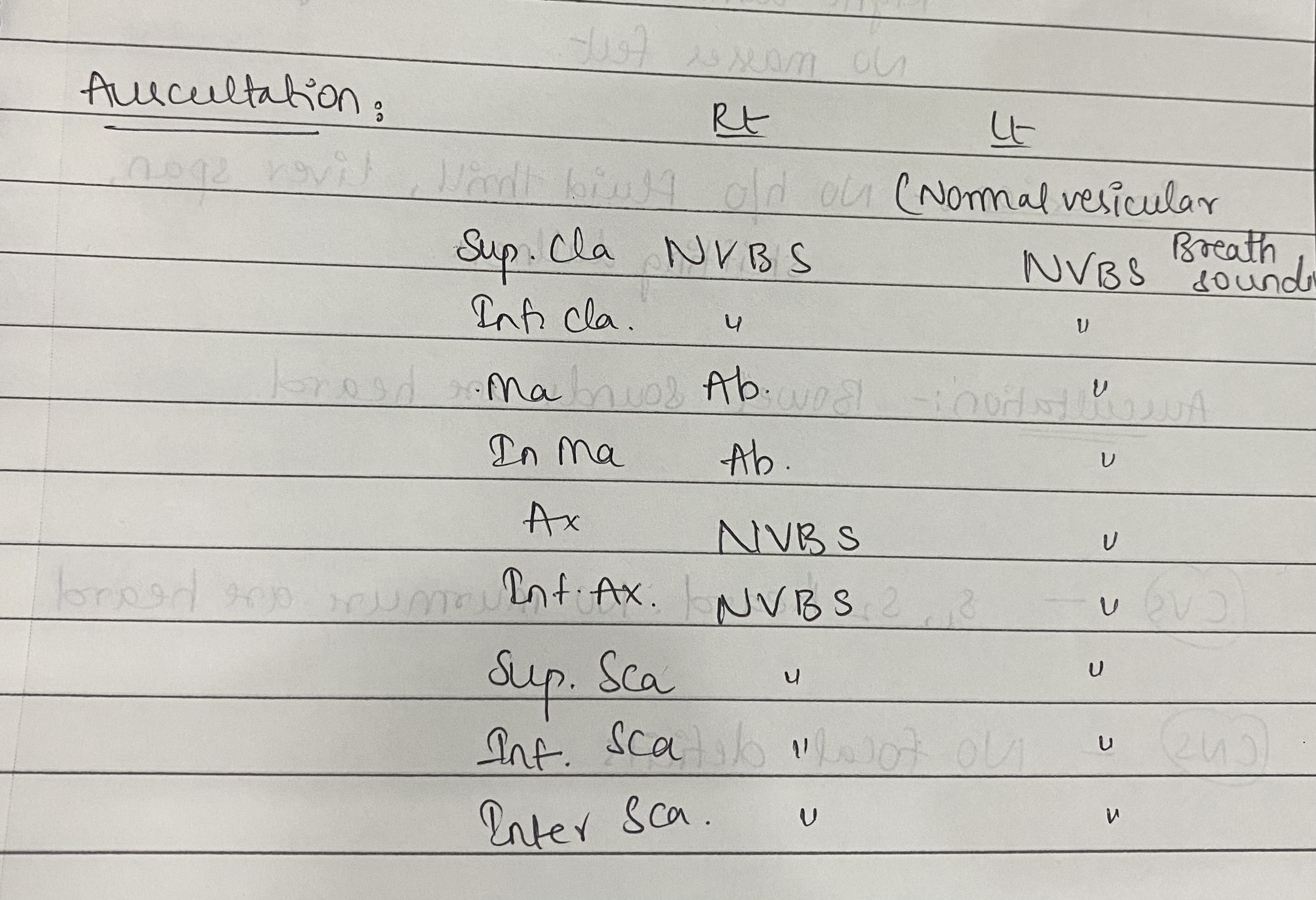
Auscultation -
Bowel sounds are heard
Cardiovascular system -
Inspection:
No chest wall abnormalities
No scars sinuses sinuses engorged veins
Trachea appears to be central
Apical impulse not visible
Palpation:
Apical impulse felt at 5th ics 1cm medial to midclavicular line
No parasternal heaves
No thrills
Auscultation:
S1 s2 heard no murmurs
Central nervous system -
Higher mental functions :intact ,normal
Cranial nerves :normal
Sensory examination: Normal sensations felt in all dermatomes
Motor examination: normal tone,power in upper and lower limbs, normal gait
Reflexes: B/l elicited
Cerebella’s function: normal
No meningeal signs were elicited
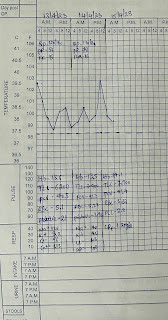
Investigations -
Fever chart
Usg report
Provisional diagnosis -
Right sided Pleural effusion sec. To TB
Mild hepatospleenomegaly
Treatment:
Iv fluids NS
Inj neomol 1gm iv
Inj tramadol 1amp in 100 ml of NS
Inj pan 40mg
T.azithromycin 500mg
Tab ATT
4 tabs H 340mg,R 680mg,Z 1700mg,E 1020mg
Tab PCM 650mg
Syrup grilintus 15ml
Tab pyridoxine 25mg
Inj diclofenac I.m













Comments
Post a Comment